Thanks for reading Sex Matters News! Subscribe for free to get new posts.
It will involve 226 children under 16 being given puberty blockers that will stop them maturing physically, mentally and reproductively while they are on the drugs, setting them up for a pathway of further medicalisation with cross-sex hormones. The impact on their health will be monitored for just one or two years under the trial protocol.
The primary measure of outcomes is the “Kidscreen 10” test, in which the children will be asked questions such as “Have you felt full of energy?” and “Have you had fun with your friends?”.
Promoters of the trial say:
“Gender incongruence is often a lifelong condition in which the ultimate aim of intervention is to promote long-term well-being and good psychosocial and psychosexual functioning over the life-course.”
Yet the trial will only measure short-term outcomes, and there is nothing in the published protocol that suggests it has got to grips with the impossible promise being made to these children and their families: that they can truly live life as if they were the opposite sex.
MPs, doctors, parents, detransitioners and campaigners are speaking up against the study on medical and ethical grounds, and considering how to challenge it on regulatory and legal grounds.
The medical ethics arguments against such a trial are well rehearsed. As the recent report on Treatment for Pediatric Gender Dysphoria produced by the US Government’s Department for Health and Human Services (HSS) says:
“The natural history of pediatric gender dysphoria is poorly understood and decades of research has shown that early-onset gender dysphoria usually resolves without medical intervention.There is no compelling evidence that the same will not prove true in the case of adolescent-onset symptoms, and limited evidence suggesting it will. And in any case, it is widely acknowledged that clinicians are unable to distinguish patients whose gender dysphoria will persist from those whose gender dysphoria will resolve. Further, there are concerns about the role medicalization itself may play in contributing to the persistence of the conditions being treated, and less invasive and less risky interventions are available. Lastly, medical intervention has known and plausible harms, and decades of research conducted by leading academic institutions have failed to produce reliable evidence of medical benefit.”
Extreme gender non-conformity in young children has long been observed to be associated with growing up to be same-sex attracted. Blocking the puberty of these children, and taking away their adult sexual function, has been dubbed “transing away the gay”.
There is another reason why this trial should not go ahead. It is based on doctors’ wishful thinking, bordering on reckless, about the degree to which other people, and institutions, can be forced to accept a person “as the opposite sex”. This is the issue about “social transition” that we called on Dr Hilary Cass to consider, but were told was outside her mandate.
Following the For Women Scotland Supreme Court judgment the issue is even clearer. Expectations of socially transitioned life have long rested on a misunderstanding of Section 9(1) of the Gender Recognition Act, which granted a person the right to be recognised as the opposite sex “for all purposes”. The Supreme Court has now found that section 9(1) has a much more limited effect than many previously assumed.
In particular, it concluded that separate-sex services are provided on the basis of biological sex, and that protection against sex discrimination and harassment relate to biological sex. This means that people cannot use the law to force “acceptance” that they are the opposite sex on others in the way they had hoped, no matter what medical interventions they undergo.
On 28th April, together with Transgender Trend, LGB Alliance and Genspect, we wrote to Sir James Mackey, the CEO of NHS England, and Wes Streeting MP, Secretary of State for Health and Social Care, explaining the implications of the Supreme Court judgment and asking them to cancel the trial. We wrote:
“The drugs are intended to block gender-distressed children’s natural puberty so that if they persist in cross-sex identification and progress to cross-sex hormones and perhaps surgery, they will “pass” better as the opposite sex. But passing as the opposite sex ceases to be a desirable goal to present to children when they will never be permitted to use spaces or services for the opposite sex, and may in future be restricted in employment in roles such as police officer or nurse which can involve intimate contact with others in situations where sex matters for those others’ human rights. Instead it becomes a major, permanent social problem for those young people, since their future lives and freedoms will be seriously curtailed by being legally barred from using the other sex’s spaces while appearing anomalous in those for their own sex.”
But now the trial is proceeding, and the protocol published last week reveals that the framework for obtaining assent/consent of children and their parents does not address the legal constraints on transition. It simply swerves the question of whether children’s and parents’ expectations are realistic and informed.
“Gender incongruence”: a desire classified as a medical condition
The stated aim of the study is to evaluate benefits and risks of using gonadotropin releasing hormone analogues (GnRHa) for puberty suppression in children and young people with “gender incongruence”.
This term comes from the World Health Organisation’s International Classification of Diseases (ICD-11), in which the condition was reclassified from a mental-health issue (“gender identity disorder”) to sexual health in 2022, in order to reduce stigma concerning accessing “gender affirming healthcare” (notwithstanding there is no good evidence base for this care). It is framed in the language of gender ideology.
The Pathways protocol says:
“Gender incongruence is characterised by a marked and persistent disparity between an individual’s experienced gender and the birth-registered sex, which may lead to a desire to ‘transition’, to live and be accepted as a person of the experienced gender. Gender incongruence may be more distressing during significant transitional life stages such as adolescence, which can lead to gender dysphoria.”
The diagnosis of gender incongruence or gender dysphoria is based entirely on subjective self-reports and behavioural observation. It centres on attitudes, feelings, and behaviours that are known to fluctuate during adolescence. The logic of the diagnosis and treatment pathway is circular. The condition is based on “a desire to ‘transition’”. Treatment for the condition is offered as the means to do ‘transition’, whatever that may mean.
The Pathways study, like the Cass Review before it, pays little attention to the practicality of hoped-for social transition in a world with rules and laws that relate to sex and other people, who also have rights.
It can be dangerously easy to glide past these difficulties when talking about mentally distressed pre-pubescent children and adolescents. The study protocol says:
“Social transition refers to changes in the way the child or young person lives that align more closely with their experienced gender, including changes to their appearance, clothing, name, pronouns or behaviour, for example.”
It says nothing about whether they are allowed (currently or in the rest of their school career) to use opposite-sex toilets, showers and changing rooms, whether they are allowed to compete as the opposite sex in sports, what happens on school trips, whether other children, parents and teachers will be told the truth about what sex they are, and whether others will be forced to use their preferred pronouns.
Nor does it say anything about how their hopes might play out in the future, in the adult world of work, romance, leisure, family and service use. Women’s refuges, prisons, searching, rules on data accuracy and the law on sex by deception are topics far beyond the understanding of children who believe they were “born in the wrong body”.
The approach of blocking puberty in children was developed by doctors after the medical treatments pioneered to meet adults’ desire to live “as the opposite sex” yielded disappointing outcomes. Doctors in the Netherlands hypothesised that the results of such “sex change” procedures would be more successful if they could be done on patients who had been prevented from developing secondary sexual characteristics in the first place, so that they would be better able to “pass” as the opposite sex.
However, there was never good evidence or ethical justification for the practice based on considerations of child development.
And the FWS judgment has made clear that the ability to live as if you are the opposite sex (rather than the freedom to live as a gender non-conforming member of your own sex) is limited. An individual’s rights in this respect do not change depending on how well they pass.
Are you mainly a boy or mainly a girl?
The inclusion criteria for the study include that the child or young person meets diagnostic criteria for gender incongruence according to ICD-11. Specifically:
The child or young person has a strong desire to be a different gender than the assigned sex;
The child or young person has a strong dislike of sexual anatomy or anticipated secondary sex characteristics;
The incongruence has persisted for a minimum of 2 years;
The child or young person has a strong desire to “transition”, to live and be accepted as a person of the experienced gender.
The clinician leading on care must consider that there is a “reasonable prospect of benefit”. This benefit might be achieved in relation to quality-of-life parameters (for example, confidence in peer and family relations, participation in school and/or leisure activities, improved sense of well-being), mental or physical health.
The child or young person and at least one parent must demonstrate sufficient understanding of the possible advantages and disadvantages of the proposed treatment including immediate psychological and physical impacts and also long-term implications, benefits and harms in the context of their personal situation and needs.
The trial protocol sets out two simplistic data-collection tools by which it will assess a child’s gender identity and keep track of their “social transition”.
The gender identity questionnaire to be undertaken at baseline, four weeks and two years asks a child or young person what best describes their gender identity:
definitely a boy mainly a boy definitely a girl mainly a girl neither a boy or girl not sure none of the above.
Those aged over 12 will be asked about other words they use to describe their gender identity:
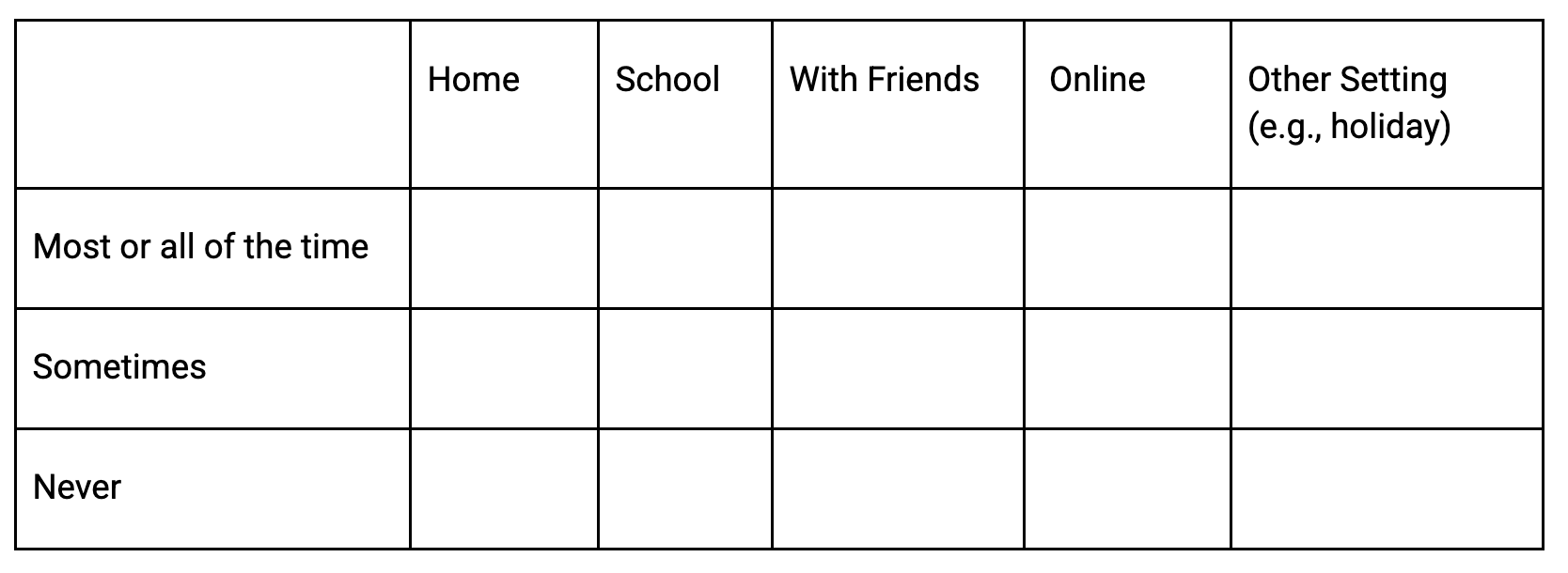
A Social Transition Questionnaire will be administered at the same time. Children will be asked:
Have you socially transitioned in any of the following settings?
While there is significant emphasis on discussions of fertility preservation, there is nothing in the protocol requiring legal and practical constraints on transition to be explained or understood by children and parents, or even by the clinicians undertaking the study.
These tricky questions are someone else’s problem.
“Was the Equality Act meant to treat a trans woman with a gender recognition certificate as a woman? And we came unanimously to the view that it didn’t. Did we realise that would cause an outrage for people? Yes, because people had been led to believe by public authorities, among others, for the last 15 years that they had rights which they didn’t have. So I have some sympathy, quite a lot of sympathy, with the feeling that they had something taken away from them.”
Children as young as nine, and their parents, are being asked to agree that they have considered the “long-term implications, benefits and harms in the context of their personal situation and needs” without being given any guidance for this, in the context where they have been told that following the law is “transphobia” and that they have rights they do not in fact have.
Meanwhile government departments that have promoted misunderstanding of the law for the past 15 years have gone into hiding. The Office for Equality and Opportunity is not willing to say clearly what the Equality Act says for single-sex services, and the Department for Education has failed to produce guidance for schools on what to do when a child says they wish to undertake “social transition”.
The Department of Health, NHS England, the National Institute for Health and Care Research and the Research Ethics Committee which approved this study have allowed it to go ahead by ignoring the conflict with the Equality Act and feeding the unrealistic hopes of children who are not old enough to understand or consider these constraints on their desires.
Recruiting children into a study that is based on a mis-selling of rights and which forecloses their chances for adult sexual function and fertility is unconscionable. It is a breach of the Good Clinical Practice necessary for a lawful trial. We have written to Wes Streeting again urging him to stop the trial.
Thanks for reading Sex Matters News! Subscribe for free to get new posts as they are published.